Rohingya refugees in Jammu are falling through India’s TB system

Rohingya refugees in Jammu are falling through India’s TB system
Overcrowded settlements, poor living conditions and the absence of recognised identity documents are delaying tuberculosis diagnosis and interrupting treatment for Rohingya refugees living in Jammu.
Jammu, Jammu and Kashmir: Every morning, Hamid Hussein (name changed), in his thirties, steps out of the makeshift tent he shares with his family in Kiryani Talab, a Rohingya refugee settlement in Jammu district’s Narwal area, to look for daily wage work, even as his body struggles to keep up. Diagnosed with tuberculosis in September 2025, Hussein completed a six-month course of treatment at a private hospital, but told 101Reporters that weakness and irregular work now make survival itself uncertain.
Kiryani Talab, home to more than 100 Rohingya refugee households living in temporary shelters along the roadside, offers little protection from heat, rain or disease. Overcrowding, poor sanitation, limited ventilation and precarious access to healthcare have left many residents vulnerable to illnesses such as tuberculosis (TB).
 Piles of garbage lying outside an informal settlement in Bathindi, Jammu, underscoring the poor sanitation conditions faced by residents (Photo - Urvat Il Wuska , 101Reporters)
Piles of garbage lying outside an informal settlement in Bathindi, Jammu, underscoring the poor sanitation conditions faced by residents (Photo - Urvat Il Wuska , 101Reporters)
The Rohingya, a persecuted Muslim minority from Myanmar, have fled decades of violence and displacement, with many seeking refuge in countries such as Bangladesh and India. An estimated 40,000 Rohingya refugees currently live in India, mainly in Jammu, Delhi and Hyderabad, often in informal settlements with limited access to public healthcare systems.
Hussein arrived in India in 2017 with his wife and son, and later contracted TB at the refugee settlement. Unable to access free treatment at a government hospital due to his refugee status, he sought care at a private hospital in Gandhi Nagar, where he spent nearly Rs 40,000 on treatment. The course involved four medicines — six pills a day for the first four months, followed by four pills a day for the next two — draining the family’s limited savings and leaving him unable to afford follow-up visits.
“I have four children,” Hussein said. “No father can bear to see his children starve in front of him. Even my elder son, Najeem (11), had to drop out of school because we couldn’t pay his fees. I feel very weak, and I only get to work two or three days a week. I don’t know how we will manage now.”
Hussein said that his wife Hajira’s earnings during the walnut and almond nut-cracking season, which were around Rs 250 a day, helped the family cobble through while he underwent treatment. But much of that income went towards medicines, hospital visits and household expenses, leaving little behind for food or savings.
“Now that the season has ended, we are struggling even for basic needs,” he said. “How can we even think about hospital follow-up treatment?”
While India’s National TB Elimination Programme (NTEP) guarantees free diagnosis and treatment, many Rohingya refugees in Jammu say the absence of Aadhaar cards and other recognised identity documents prevents them from accessing government healthcare services. This remains the case even for the 22,500 Rohingya in India who are registered with the United Nations High Commissioner for Refugees (UNHCR).
Documentation barriers
Noor Bano (name changed), in her forties, who arrived in India in 2017 with her husband Raheemullah and their two sons, said that her TB treatment was delayed because she could not furnish the documents demanded by hospital authorities.
“We are registered with UNHCR, but we don’t have Aadhaar cards or the other documents government hospitals ask for,” she said. “So either we live with the illness or spend whatever we earn at private clinics.”
Bano said her illness began with a persistent cough, which she initially treated with medicines from a local chemist.
“At first, I thought it was a minor infection. But when it got worse, I went to a government hospital and was diagnosed with TB,” she said. “When they asked for Aadhaar and identity documents for treatment, I had to return home.”
 Noor Bano with her husband inside their jhuggi in the Bathindi settlement of Jammu, where the family continues to navigate life amid limited living conditions and healthcare access; (below) Aerial view of a Rohingya refugee settlement near Kiryani Talab in Narwal, Jammu, where families live in densely populated informal shelters with limited basic services (Photo - Urvat Il Wuska , 101Reporters)
Noor Bano with her husband inside their jhuggi in the Bathindi settlement of Jammu, where the family continues to navigate life amid limited living conditions and healthcare access; (below) Aerial view of a Rohingya refugee settlement near Kiryani Talab in Narwal, Jammu, where families live in densely populated informal shelters with limited basic services (Photo - Urvat Il Wuska , 101Reporters)

“I wanted to start treatment. First, my identity did not allow me to get it, and then my destiny,” she added. “Just when my husband managed to save some money, he was diagnosed with a hernia and needed surgery. His treatment had to come first, so I went back to relying on medicines from nearby pharmacies for temporary relief.”
Anwara (32), a community health worker who works with Rohingya families in Jammu, said the community is highly vulnerable to tuberculosis due to overcrowded living conditions and a lack of proper ventilation.
Overcrowded settlements
Another Rohingya refugee, Rahmat Ali (name changed), in his forties, told 101Reporters that in most shelters, eight to ten persons live together in a crammed space.
“There is garbage right outside the jhuggi…we have no proper toilets or drainage systems, so when one person falls sick, the entire family lives in constant fear of getting infected,” Ali said.
Bano added that severe water shortages and poor sanitation make even basic hygiene difficult in the settlements.
“We spend hours waiting in long queues to buy water from tankers that come only once or twice a week. For the rest of the week, the same water must be managed for drinking, cooking, bathing and cleaning. Sometimes there is such a shortage that we cannot bathe for two or three days,” she said.
 Plastic cans lined up by Rohingya Refugees to buy water from tankers in an informal settlement in Bathindi, Jammu, highlighting their daily struggle for access to clean water (Photo - Urvat Il Wuska , 101Reporters)
Plastic cans lined up by Rohingya Refugees to buy water from tankers in an informal settlement in Bathindi, Jammu, highlighting their daily struggle for access to clean water (Photo - Urvat Il Wuska , 101Reporters)
Not only do these overcrowded and unsanitary living conditions increase the risk of tuberculosis transmission, but they also make recovery more difficult for patients already weakened by the disease, especially amid poor nutrition and inadequate rest.
Anwara added: “Despite living in a high-risk environment, language barriers, unstable incomes and lack of documentation delay and interrupt treatment and diagnosis.”
According to the World Health Organization, nearly half of all untreated TB cases can prove fatal. Medical experts warn that interrupted or incomplete treatment also increases the risk of multidrug-resistant (MDR) and extensively drug-resistant (XDR) tuberculosis, which are forms of the disease that are far more difficult and expensive to treat.
Challenges in accessing healthcare
According to Jaffar Alam (32), a community leader from a Rohingya settlement near Bathindi, even in cases where refugee cards are accepted for basic consultations or emergency care on humanitarian grounds, the indirect costs of treatment remain difficult to bear.
“Transport to clinics, lost wages from taking time off work, and repeated hospital visits create enormous economic strain. For a daily-wage earner, missing even a single day’s income can mean less food on the table,” he said.
Mohammad Hussain, a community leader from Sujwan settlement, said, “The only way to earn money here is through daily wage jobs like construction labour, scrap collection, rag-picking and recycling.”
“On average, a household survives on Rs 8,000 to Rs 10,000 a month, but nearly half of it goes towards rent. Then there are electricity bills, water expenses, food, medicines and school fees for children,” Hussain said.
Anwara added that the fear of detention or deportation also discourages many refugees from seeking diagnosis or continuing treatment.
“The risk of detention and legal consequences creates deep mistrust towards public institutions, including healthcare systems,” she said. “As a result, people may hesitate to access them, sometimes even interrupting treatment in order to remain invisible to the system.”
Beyond this, refugees living with TB also described the emotional toll of the disease. Ayesha Begum (name changed), in her fifties, said she struggled to remain emotionally strong throughout her treatment. “After my husband passed away, I was left alone with no one I could truly share my feelings with,” she said. “I often feel isolated because I cannot openly tell people that I have TB. Once people know, they begin to look at you differently.”
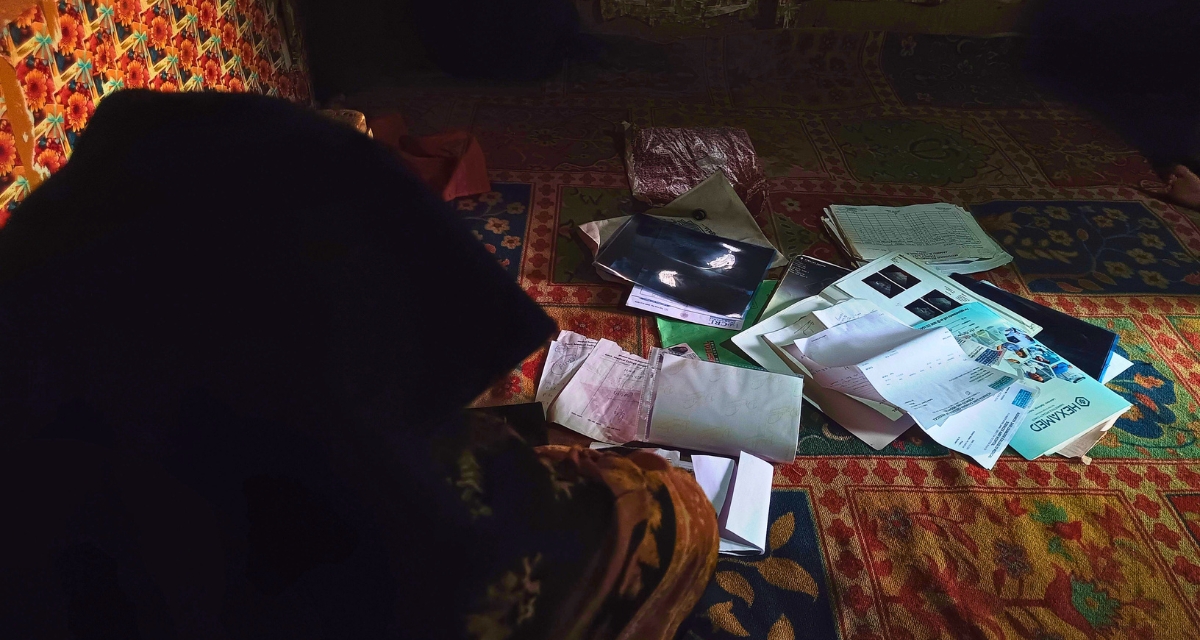 Ayesha Begum while sitting inside her shelter in an informal settlement in Jammu, beside her medical prescriptions that reflect her ongoing struggle to access consistent healthcare (Photo - Urvat Il Wuska , 101Reporters)
Ayesha Begum while sitting inside her shelter in an informal settlement in Jammu, beside her medical prescriptions that reflect her ongoing struggle to access consistent healthcare (Photo - Urvat Il Wuska , 101Reporters)
Family members said misconceptions surrounding TB often lead people to avoid patients diagnosed with the disease, forcing many to conceal their illness even in overcrowded settlements where privacy is limited.
“Mental health challenges among TB patients are often overlooked, especially in vulnerable refugee communities where survival becomes the first priority,” said Dr Asim Andrabi, a Jammu-based public health specialist working on TB and mental health. “When mental health is ignored, it directly affects treatment adherence and recovery.”
Nayla Hashmi (37), an independent human rights activist based in Jammu who works with displaced and vulnerable communities, said displacement and prolonged legal uncertainty place an additional psychological burden on refugees trying to access healthcare.
“When services are not designed to reach people living at the margins, they remain out of reach in practice,” she said. “Denying healthcare to refugees is a violation of both constitutional and international human rights obligations…The right to health is protected under Article 21 of the Constitution of India as well as the Universal Declaration of Human Rights. Refugees are entitled to the same standard of care.”
Meanwhile, Babar Baloch, spokesperson for the United Nations High Commissioner for Refugees, said, “We continue to work closely with authorities and health partners to help ensure that no one is left behind in accessing life-saving healthcare, regardless of nationality, legal status or documentation.”
Cover Image - One of the Jhuggis in Bhatindi, Jammu, reflecting the harsh living conditions faced by Rohingya refugees (Photo - Urvat Il Wuska , 101Reporters)
Would you like to Support us
101 Stories Around The Web
Explore All News